

Read “A decade of hospital costs for firearm injuries in the United States by region, 2005-2015: government healthcare costs and firearm policies” in Trauma Surgery & Acute Care Open (published April 8, 2022)
Letter to the Senate Judiciary Committee
Our letter in support of firearm safety and violence prevention for the Senate Judiciary Committee’s Hearing on “Constitutional and Common Sense Steps to Reduce Gun Violence” on March 23, 2021.
Following the hearing, President Biden proposed a historic $5 billion investment in targeted firearm violence prevention, including support for community-based violence intervention programs.
SAFE Support for Black Lives Matter
Written by Deniz Cataltepe
Director of SAFE Medical School Chapters
SAFE: Scrubs Addressing the Firearm Epidemic was founded to rally the medical community to eliminate firearm violence with the same urgency and dedication that we have applied to exposing other health risks, such as cigarette smoking. Today, SAFE announces its support for the Black Lives Matter Movement and commits to addressing the serious public health effects of racism.
Firearm violence and systemic racism are intimately linked—Black communities are disproportionately affected by firearm homicide. In the U.S., Black people are 10 times more likely than white people to die from firearm homicide[1],[2]. Studies have shown that Black men have experienced a decrease in life expectancy of 4.14 years (compared to 2.23 years among whites) due to firearm mortality from 2000 to 2016[3]. Black women are two times as likely as white women to die from a firearm fatality due to intimate partner violence [4]. Since 2017, 82% of trans gun victims have been Black trans women [2].States with a higher calculated racism index have been found to have significantly higher Black-White discrepancies in rates of shootings of unarmed victims by the police [5].
As an organization that cares deeply about firearm violence prevention, SAFE is a staunch supporter of the Black Lives Matter movement. These disturbing, disproportionate rates of firearm homicide point to a significant racial health disparity that we cannot ignore. Systemic racism bleeds into every pocket of our communities, affecting the well-being of our Black patients through the insurmountable challenges they face in access to physical and mental health care, education, and employment. The neighborhood-level factors associated with firearm violence—lower home values, few retail and service businesses, lack of green space[6]—have been perpetuated in Black communities through decades of systemic racism in the form of redlining [7],[8].
The implicit biases we all carry have serious effects on the type of care we deliver to our Black patients,[9]with racial differences found in the use of invasive cardiac procedures [10], colorectal cancer treatments [11],and antiretroviral therapy prescription for HIV [12], to name a few [13]. Race can also be framed as an “environmental stressor,” with Black patients who report thinking about their own race at higher frequencies being found to have higher blood pressures [14]. As healthcare professionals who emphasize the value of preventive care, we must confront this epidemic at its root. It is not enough to treat our Black patients, and our patients who are victims of firearm violence, once they are rolled into our trauma bays.
One of SAFE's core aims is to support evidence-based policy and research on the epidemiology and causes of the firearm epidemic in this country. In light of the devastating losses of Ahmaud Arbery, Rayshard Brooks, George Floyd, and Breonna Taylor, as well as the deaths of multiple Black children across the country this Fourth of July weekend, SAFE will continue this effort with an unwavering sense of invigoration.
We will promote research that addresses and unpacks the systemic racial causes at the core of this issue so that our interventions can be better targeted to those in need. This includes support for violence intervention models including the Cure Violence model, in which "violence interrupters," who have close ties with neighborhoods considered most at-risk, connect with individuals in those communities; the Gun Violence Intervention, with partnerships created among faith leaders, social service workers, researchers, and law enforcement to hold “call-ins” with the small segments of communities responsible for violence; and Hospital-Based Violence Interventions, in which hospitalized young adults affected by firearm violence are connected with case workers during their hospital stay [15].
We will integrate the topic of systemic racism and its consequences on firearm violence into discussions at our medical school chapters across the country, beginning with our Stand SAFE 2020 event scheduled for this fall. We will educate ourselves and members of our national organization on the barriers posed to our Black patients by systemic racism, as well as the toll that can be taken on them by our implicit biases, which are so often hidden from our own awareness.
We will demand change from our representatives—like we have done successfully in the past with increased funding for firearm violence research—to confront police firearm violence and implement proven Violence Intervention strategies. We will work to end the loss of Black lives to senseless firearm violence.
[1]Centers for Disease Control and Prevention, CDC WONDER, “About Underlying Cause of Death, 1999-2016,” last accessed July 6, 2020, https://wonder.cdc.gov/ucd-icd10.html.
[2]Everytown, Everystat, last accessed July 6, 2020, https://everytownresearch.org/everystat.
[3]Bindu Kalesan, et al., “Cross-Sectional Study of Loss of Life Expectancy at Different Ages Related to Firearm Deaths Among Black and White Americans,” BMJ Evidence-Based Medicine 24, no. 2 (2018).
[4]Giffords Law Center, “Gun Violence Statistics,” last accessed July 6, 2020, https://lawcenter.giffords.org/facts/gun-violence-statistics/.
[5]Aldina Mesic, et al., “The Relationship Between Structural Racism and Black-White Disparities in Fatal Police Shootings at the State Level,” Journal of the National Medical Association 110, no. 2 (2018): 106-116.
[6]Michelle C. Kondo, et al., “The Association Between Urban Tree Cover and Gun Assault: A Case-Control and Case-Crossover Study,” American Journal of Epidemiology 186,no. 3. (2017): 289-296.
[7]Yasemin Irvin-Erickson, et al., “A Neighborhood-Level Analysis of the Economic Impact of Gun Violence,” Urban Institute, June 2017, https://www.urban.org/sites/default/files/publication/90671/eigv_final_report_3.pdf.
[8]Matthew Benns, et al., “The Impact of Historical Racism on Modern Gun Violence: Redlining in the City of Louisville, KY,” Injury(2020).
[9]William J. Hall, et al., “Implicit Racial/Ethnic Bias Among Health Care Professionals and its Influence on Health Care Outcomes: A Systematic Review,” American Journal of Public Health105, no. 12 (2015): e60-76.
[10]N.R. Kressin and L.A. Petersen, “Racial Differences in the Use of Invasive Cardiovascular Procedures: Review of the Literature and Prescription for Future Research,” Annals of Internal Medicine 135, no. 5 (2001): 352-366.
[11]L.F. McMahon Jr., et al., “Racial and Gender Variation in Use of Diagnostic Colonic Procedures in the Michigan Medicare Population,” Medical Care37, no. 7 (1999): 712-717.
[12]R.D. Moore, D. Stanton, R. Gopalan, and R.E Chaisson, “Racial Differences in the Use of Drug Therapy for HIV Disease in an Urban Community,” New England Journal of Medicine330 (1994): 763-768.
[13]Aaron E. Carroll, “Doctors and Racial Bias: Still a Long Way to Go,” New York Times, February 25, 2019, https://www.nytimes.com/2019/02/25/upshot/doctors-and-racial-bias-still-a-long-way-to-go.html.
[14]LaPrincess C. Brewer, et al., “Association of Race Consciousness with the Patient-Physician Relationship, Medication Adherence, and Blood Pressure in Urban Primary Care Patients,” American Journal of Hypertension 26, no. 11 (2013): 1346-1352.
[15]Giffords Law Center, “Healing Communities in Crisis,” last accessed July 6, 2020, https://lawcenter.giffords.org/wp-content/uploads/2019/01/Healing-Communities-in-Crisis.pdf.
Giffords Statement: Historic Win for Gun Safety

Congress reaches deal to fund gun violence

On December 16, 2019, Congress reached a deal to provide $25 million in funding to federal agencies studying gun violence. This deal marks the first time Congress is funding firearm violence research in over 20 years. SAFE joined Giffords and Representative Jackie Speier to fight hard for this funding at the US Capitol this past June. We are thrilled that Congress agrees it is time to research gun violence and implement evidence based strategies to save lives.
Proud to Partner with Giffords to Reduce Gun Violence
Scrubs Addressing the Firearm Epidemic-SAFE is proud to be one of the medical organizations partnering with Giffords to reduce gun violence. We are so grateful for Gabby’s courage and leadership!

Dr. Susie MacLean and Former Representative Gabby Giffords
Policies That Work to Reduce Gun Violence Conference

Our Patients, Our Lane: Why Congress Must Fund Gun Violence Research

Giffords.org: This past weekend, El Paso and Dayton were the latest American communities torn apart by gun violence. We know that these mass shootings, as well as every day gun violence, are widespread public safety issues. All Americans deserve to live without fear. We cannot let these tragedies become normalized.
A Healthcare Intervention
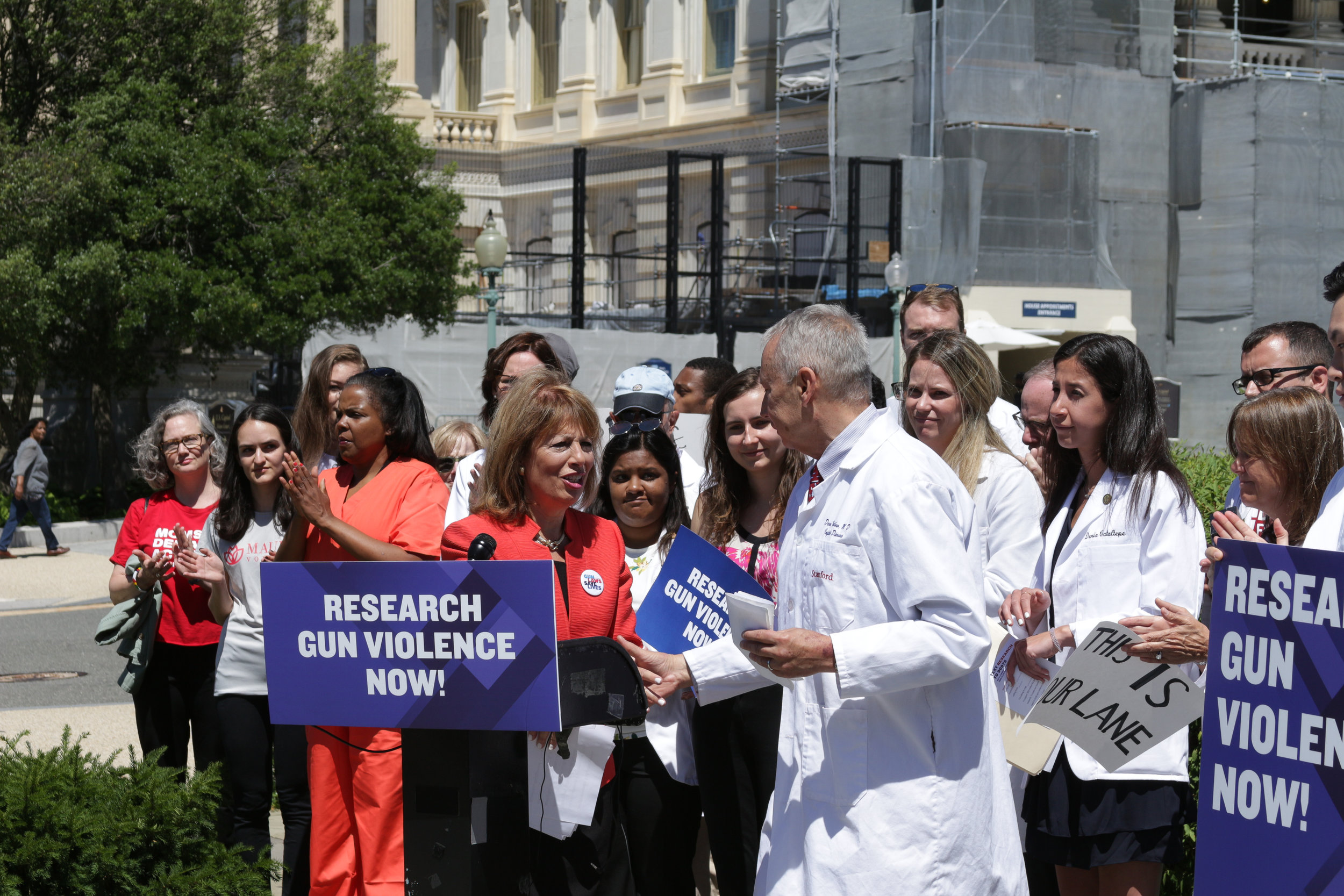
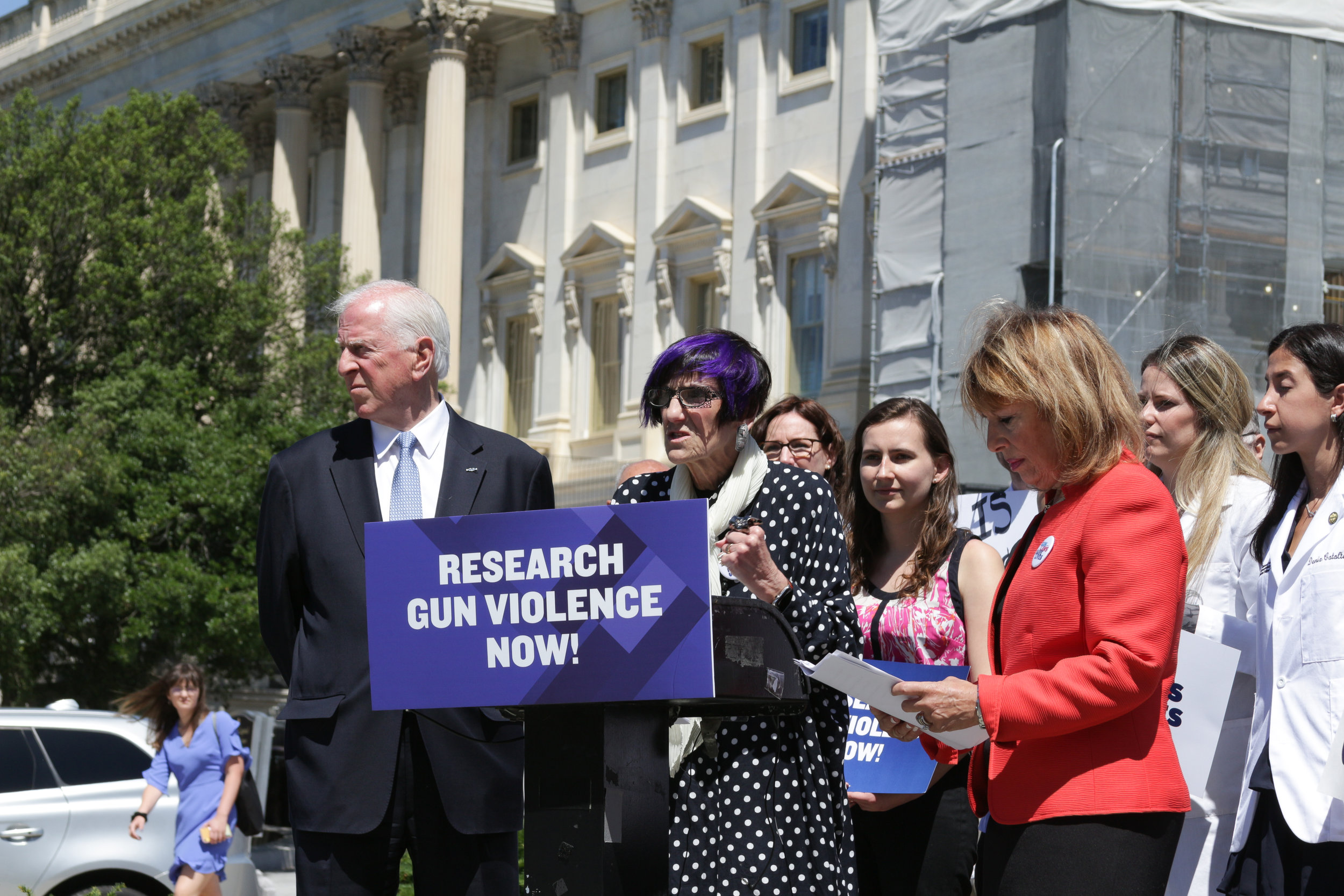
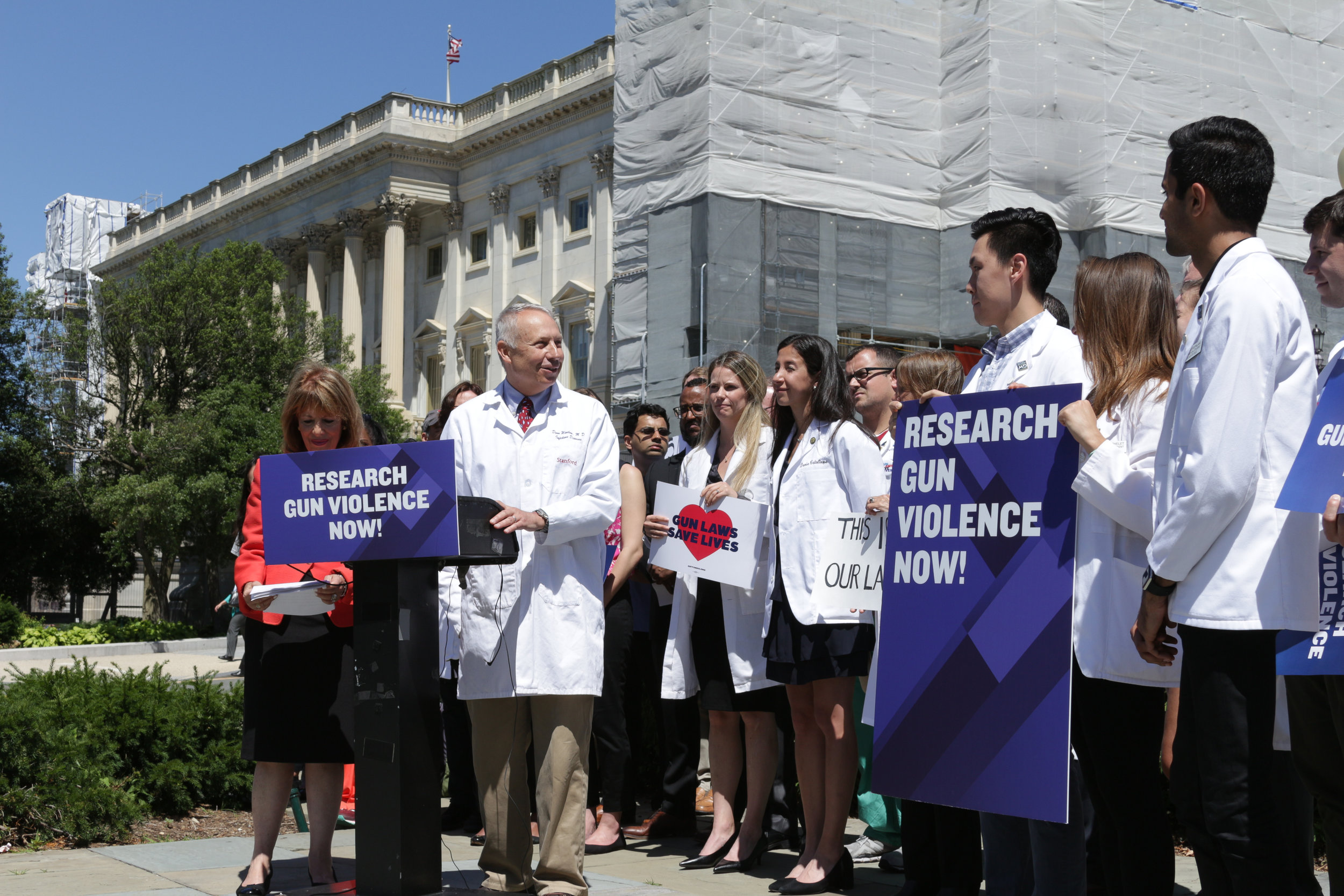
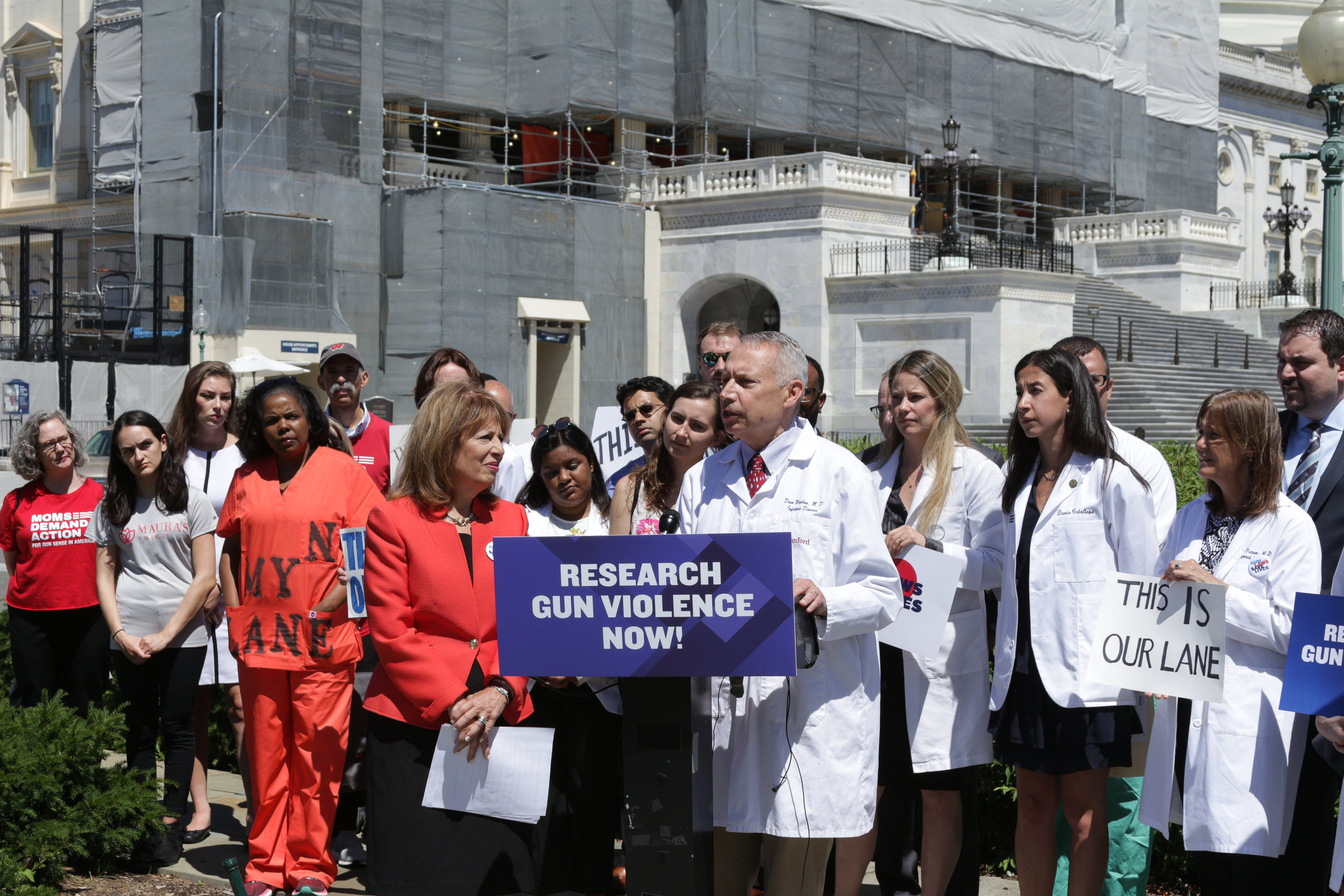
On June 11th, doctors, nurses, students and other healthcare providers, gun owners and non gun owners, Democrats, Republicans and Independents held a press conference outside the Capitol Building in order to push Congress to advance Firearms Injury Prevention Research. Watch the live video here.
Who was there?
Congresswoman Jackie Speier (CA-14)
Dr. Dean Winslow, SAFE Director; Stanford Professor of Medicine; Retired U.S. Air Force Colonel
Dr. Roger A. Mitchell Jr., Washington D.C. Chief Medical Examiner; George Washington University Clinical Professor of Pathology; Howard University Professor of Surgery
Dr. Joseph Sakran, Gun Violence Survivor; John Hopkins Hospital Assistant Professor Surgery, Director of Emergency General Surgery, and Associate Chief of the Division of Acute Care Surgery
Richard Hamburg, Safe States Alliance Executive Director
Dr. Abbie Guttennberg Youkilis, Gun Violence Survivor; Internal Medicine Specialist
Dr. Alex Grossman, UCLA Emergency Medical Resident
Along with hundreds of doctors, nurses, students and other healthcare providers; gun owners and non gun owners; Democrats, Republicans and Independents.
Why are we doing this?
Last year close to 40,000 Americans, including more than 3000 children, died from firearms injuries.
These deaths don’t happen at random. We know we can prevent gun injuries through public health research and action. Lobbyists and special interest groups in Washington are pressuring lawmakers to quash bills supporting research to protect our patients from preventable injury and death.














Medical Students Take a Stand to Stop the Bleed
April, 2019 — Will Dewispelaere, University of Colorado School of Medicine
This February medical students in Scrubs Addressing the Firearms Epidemic (SAFE) chapters across the country met with local Stop the Bleed educators to learn proper bleeding control techniques. These meetings took place as many students push for integration of bleeding control teaching into introductory medical school courses.
